Last Modified: 3/25/2024
Location: FL, PR, USVI
Business: Part B
Select “You are reporting a change to your Medicare enrollment information” in Section 1: Basic Information.
Proceed to Section 1B as noted in the far-right column.
Select “Private Practice Business Information” in Section 1B.
The column title “Required Sections” lists the sections to complete for the change as 1, 2A, 3, 4A, 12, 13 (optional) and 15 and 6 for the signer if that authorized or delegated official has not been established for this provider.
Proceed to Section 2A1.
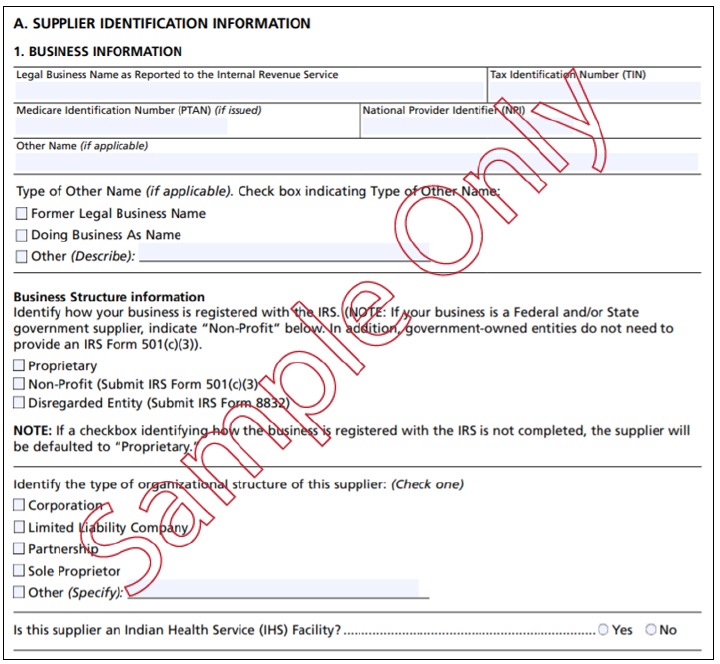
Section 2A1: Supplier Identification Information.
Section 2 is divided into Parts A through G. Complete ONLY the Business Information in Section 2A1.
Proceed to Section 3.
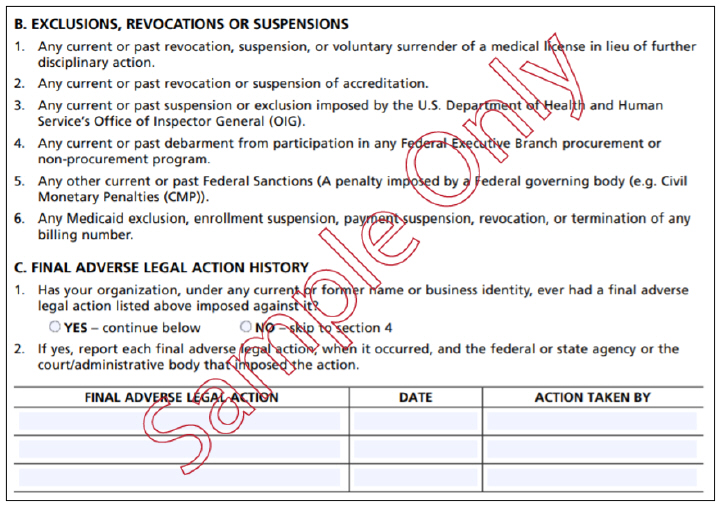
Complete Section 3 – Final Adverse Actions/Convictions.
Proceed to Section 4.
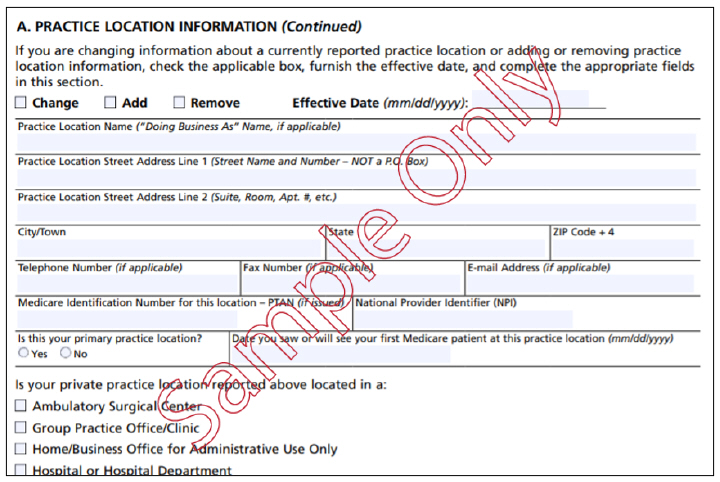
Section 4: Practice Location Information is divided into Parts A through G.
Complete ONLY THE PARTS WHICH HAVE CHANGES. For example, Section 4B pertains to Remittance Notices and Special Payments. If the information for Remittance Notices and Special Payments has not changed, the fields should remain blank. Complete the information which has changed.
Note: Prior to terminating a practice location, where the NPI linked to that location is not linked to any other practice location(s), please ensure all outstanding claims have been submitted and processed by Medicare.
Proceed to Section 13.
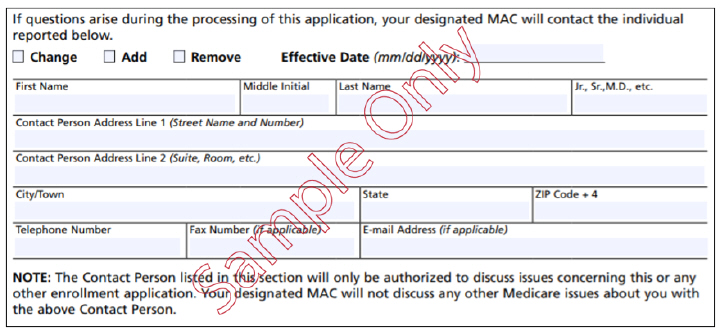
Section 13: Contact Person.
Complete the Contact Person’s information. The person will be contacted regarding the application, but if a contact person is not listed, the provider will be directly contacted.
Proceed to Section 15B.
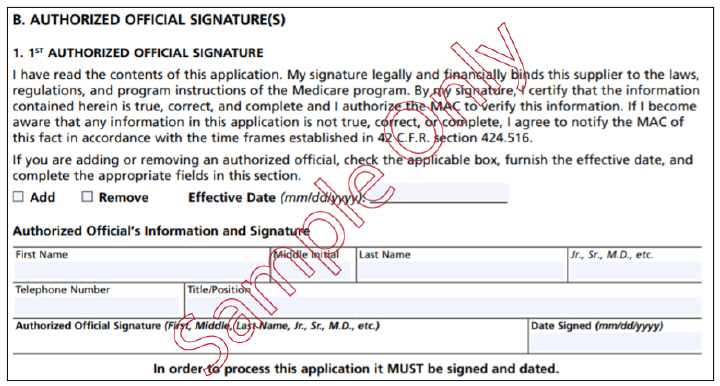
Section 15B. Certification Statement is the section in which a signature (preferably blue ink) certifies the submitted information.
The signature must be the Authorized Official’s signature.
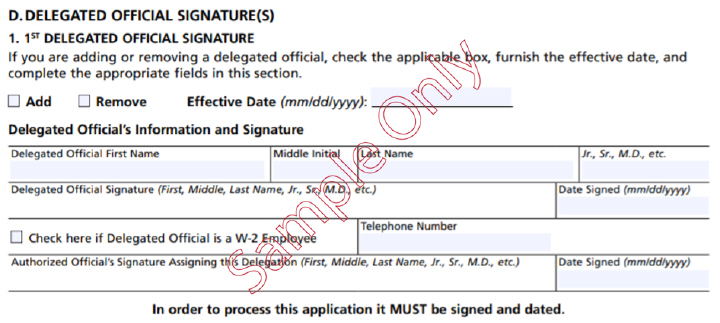
If the Delegated Official is signing, proceed to Section 15D.
Section 15D: Section 15D is provided for the Delegated Official’s Signature.
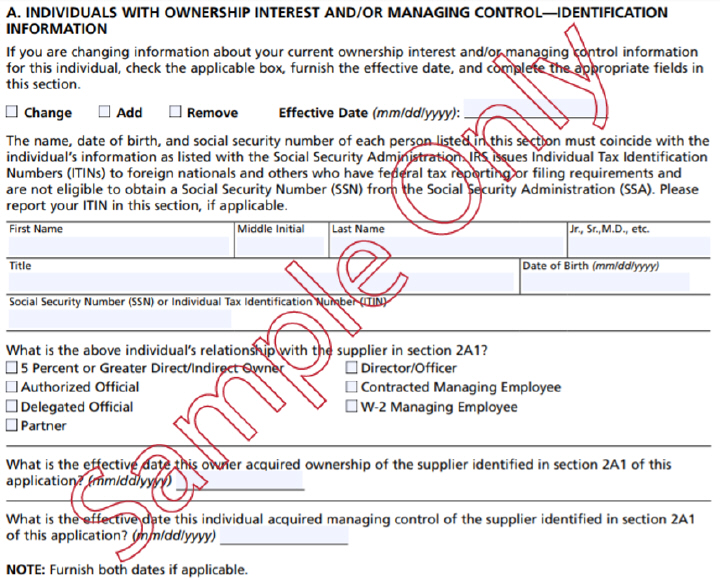
If the Authorized Official or the Delegated Official has not been established for the provider, proceed to Section 6.
Section 6: Ownership Interest and/or Managing Control Information must be completed if the Authorized Official or the Delegated Official has not been established for the provider.
If you decide to mail the application, you will need to mail the completed, signed form and all supporting documentation to First Coast Service Options. Mailing addresses can be found below:
Jurisdiction N (JN): Florida, Puerto Rico, U.S. Virgin Islands
First Coast Service Options
Provider Enrollment Services
P.O Box 3409
Mechanicsburg, PA 17055-1849
First Coast Service Options (First Coast) strives to ensure that the information available on our provider website is accurate, detailed, and current. Therefore, this is a dynamic site and its content changes daily. It is best to access the site to ensure you have the most current information rather than printing articles or forms that may become obsolete without notice.