
Instructions for completing the SPOT submitter ID update request form
The SPOT submitter ID update request form should be completed to update information on file for your existing SPOT portal submitter ID.
General information
It is important that you use the most recent version of any EDI form when enrolling for EDI services or updating your existing EDI status. Please carefully review the following block-by-block instructions to ensure successful completion.
Note: The following screenshots are for instructional purposes only and cannot be completed and submitted for enrollment.
General information

Instructions
- Select one from each drop-down depending on your location and the line of business you submit claims for.
Current provider information

Information
- This is a required block. The form will be returned if these fields are not completed accurately.
Instructions
- Type the current tax ID or the SPOT submitter ID. All SPOT submitter IDs with the same tax ID will be updated.
- Type the current legal business name.
- Type the correspondence fax number.
- Type the complete mailing address for correspondence.
Change information
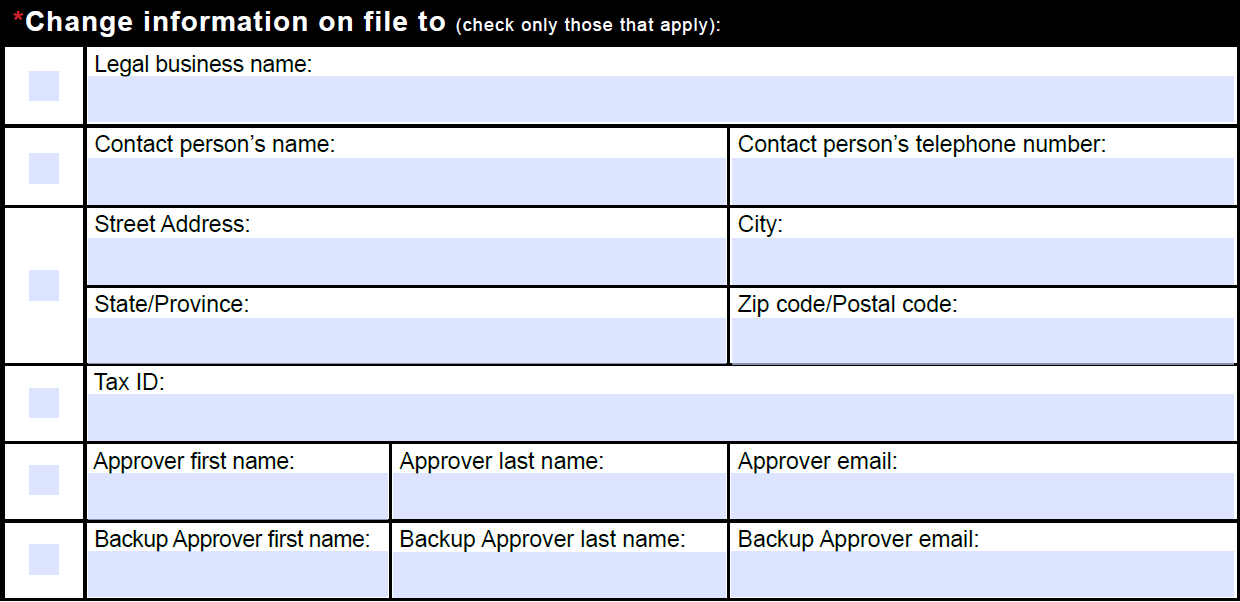
Information
Complete only the information that needs changed from the existing SPOT account information. At least one completed row is required.
Instructions
Legal business name
- To change the legal business name, check this box and type the new legal business name
Contact person’s name
- To change the contact person information, check this box and type the new contact person’s full name and complete telephone number.
Street address
- To change the organization’s street address, check this box and type the new street address, City, State, and ZIP code.
Tax ID
- To change the organization’s Tax ID, check this box and type the new Tax ID.
Approver
- To change the organization’s office approver, check this box and type the new approver’s first name, last name, and email address.
Backup approver
- To change the organization’s office backup approver, check this box and type the new backup approver’s first name, last name, and email address.
Required signature
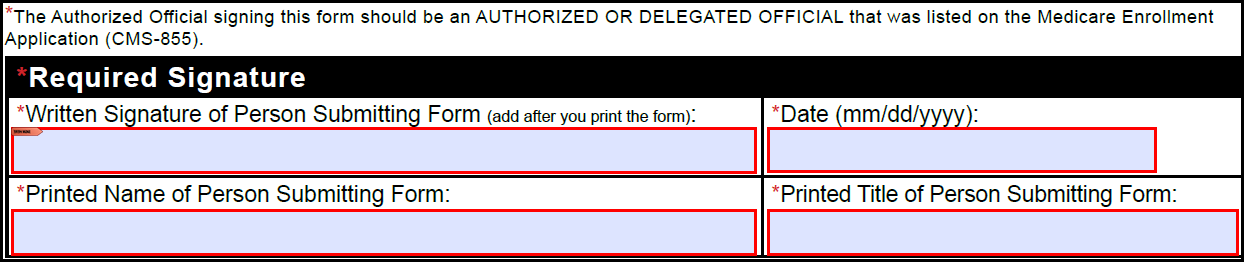
Information
This is a required block. The form will be returned if any of these fields are not completed accurately.
The organization’s authorized or delegated official should complete this section with their printed name and title, then sign and date the form.
Instructions
- Review the entire form to verify the information provided is accurate and complete.
- Type the date the form was signed. The date must be a full month, day, and year.
- Type the printed name of the person signing the form.
- Type the professional title of the person signing the form.
- Print the form.
- Sign in the written signature block with a black or blue ink pen.
- Email the form to MedicareEDI@FCSO.com or fax to 904-361-0470.
- Allow 10 business days for processing.