Targeted probe and educate (TPE) round results: Rehabilitation services outpatient
Top denial / partial denial reasons and high-level results are listed below from each round of rehabilitation services outpatient TPE reviews that have been conducted thus far by Medical Review. If you have questions about your individual results, please contact the nurse reviewer assigned to your review for additional information. Additional rounds of review will be utilized when the targeted topic demonstrates a continued need for review with newly identified providers.
Top denial / partial denial reasons
The most common reasons for denial or partial denials are the following:
- Medical necessity - The documentation submitted does not support medical necessity as listed in coverage requirements.
- Insufficient documentation - Insufficient documentation was provided to support the services as billed to Medicare. Medical Review makes multiple attempts to correct these error types before completion of the review. Below are the following denial reasons for insufficient documentation that we were not able to resolve:
- Documentation submitted did not support the number of therapy minutes / units billed.
- Documentation submitted was insufficient to support the plan of care.
- Documentation submitted lacked a signed certification / recertification.
- Documentation submitted did not support a valid plan of care.
- Documentation submitted did not support the service was provided by PTA but was incorrectly billed.
- Documentation submitted lacked evidence that the service was performed by the required expertise of the licensed therapist.
- Documentation submitted lacked a valid signed plan of care.
- Documentation submitted lacked an initial evaluation.
- Documentation submitted did not support the reason for delayed / lacked (re)certification.
- Documentation submitted lacked all required elements for the service billed.
- Documentation submitted did not support the plan of care was established and signed by a qualified clinician/practitioner.
- Documentation submitted did not support the appropriate supervision by a qualified clinician/professional.
- Documentation submitted did not support certification/recertification of the plan of care.
- Documentation submitted lacked an evaluation and progress note.
- Documentation supports the CQ and/or CO modifier should have been billed as services furnished in whole or in part by a therapy assistant.
- Documentation submitted did not support the approval/certification of the plan of care for the therapy services.
- Documentation submitted did not include a progress report which was completed a minimum of every 10th treatment visit throughout the episode of care or within 7 calendar days from the end date of the reporting period.
- Documentation did not include a treatment not which contained all the required elements.
- Non-response to documentation requested.
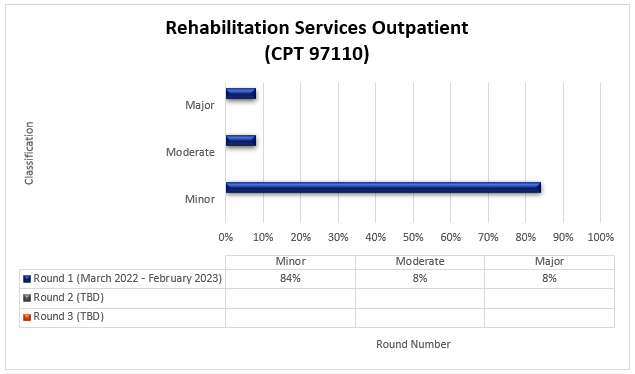
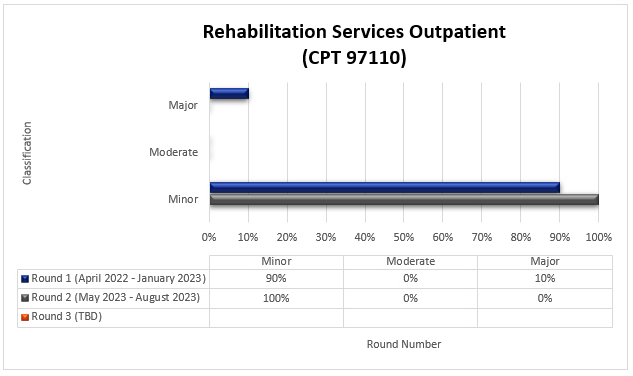
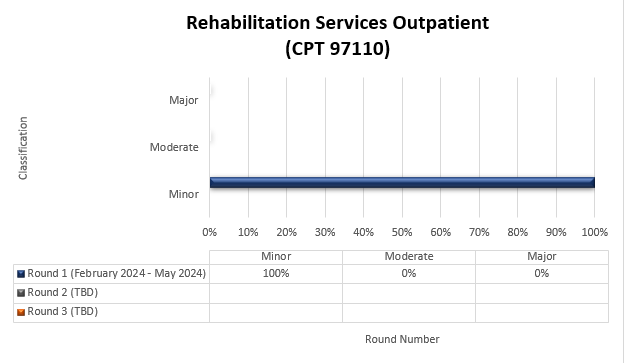
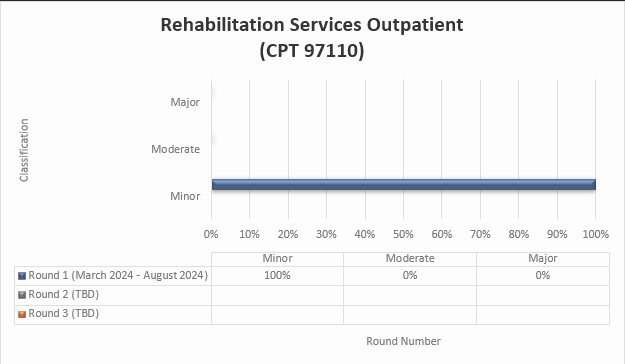
Round results
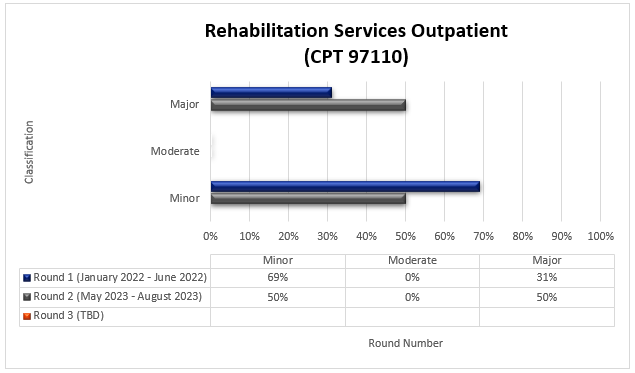
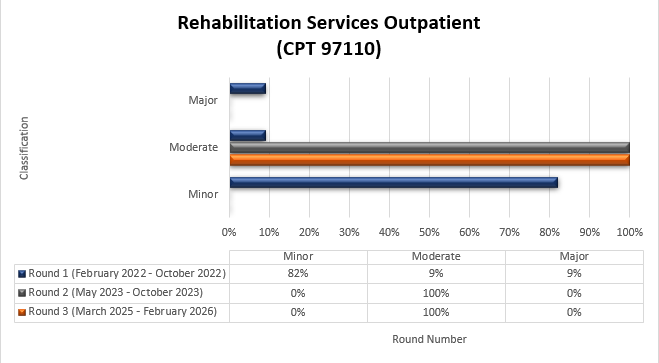
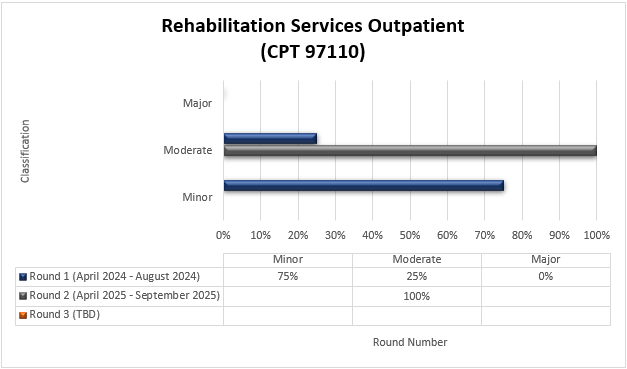
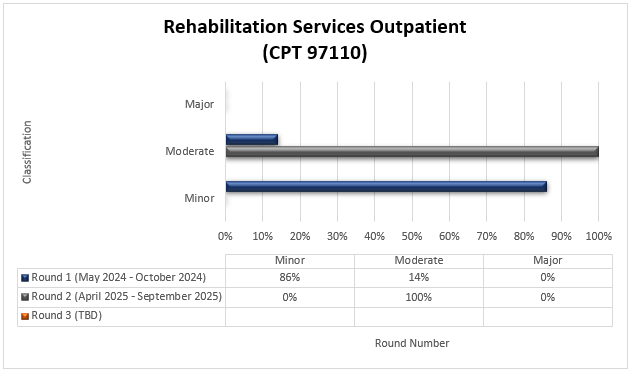
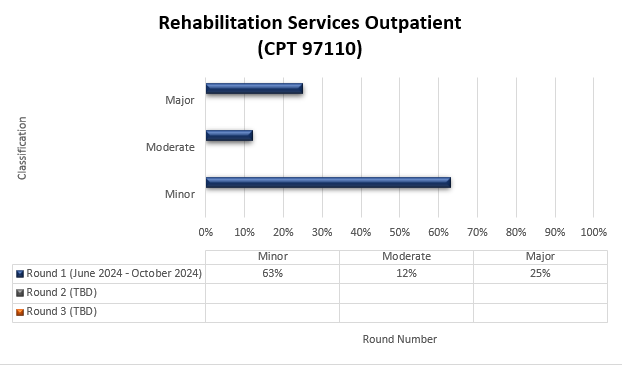
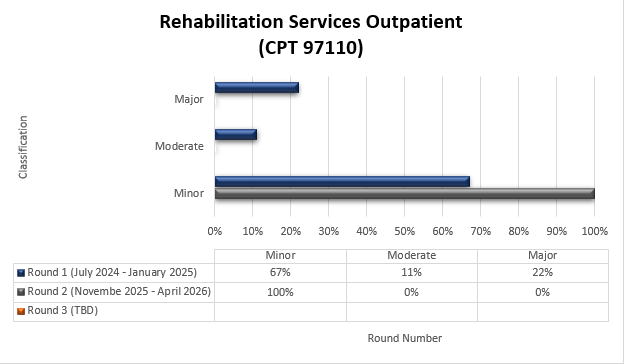
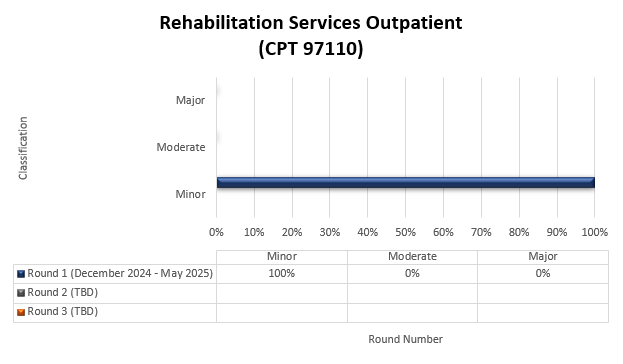
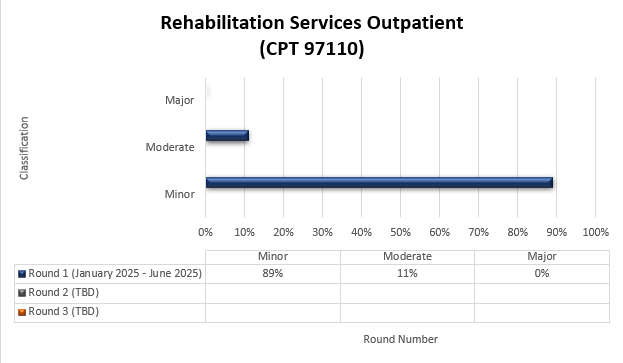
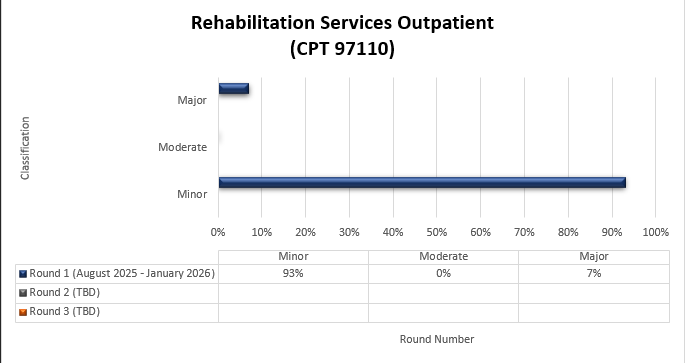
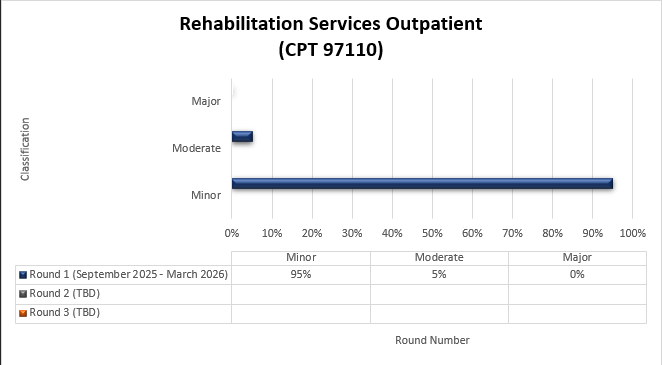
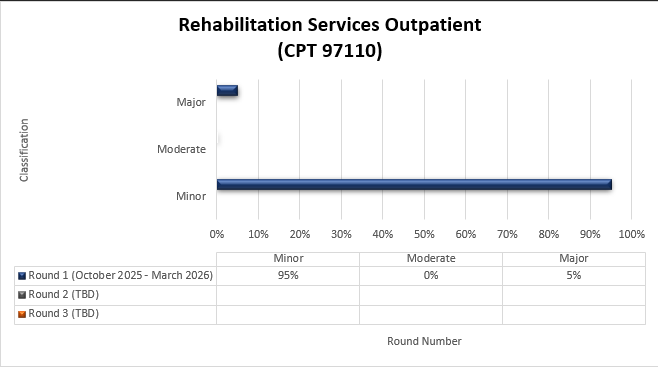
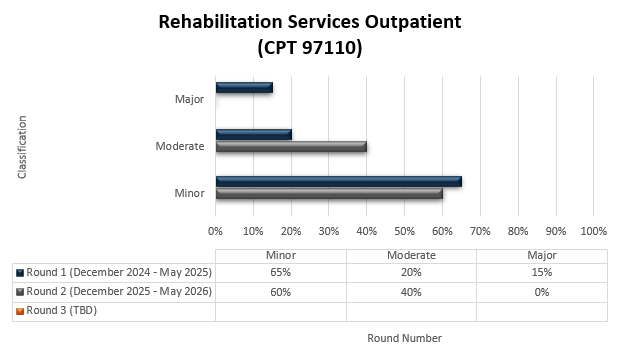
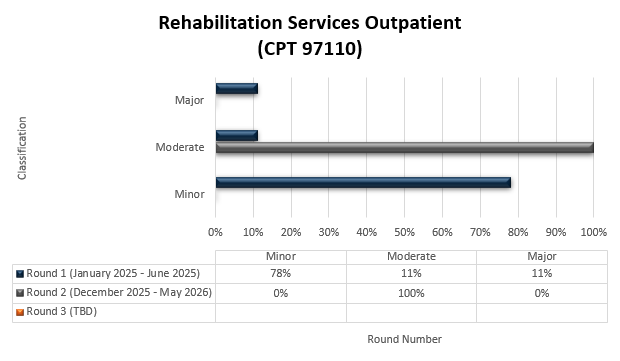
CPT 97110
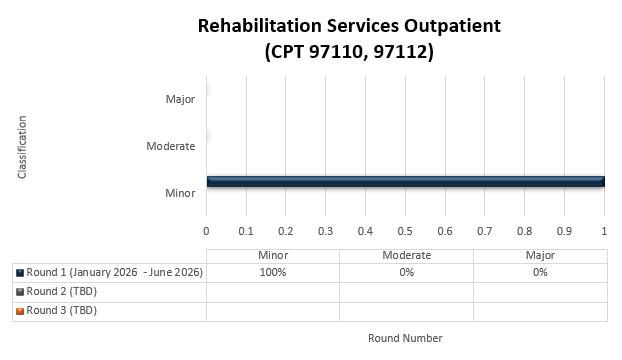
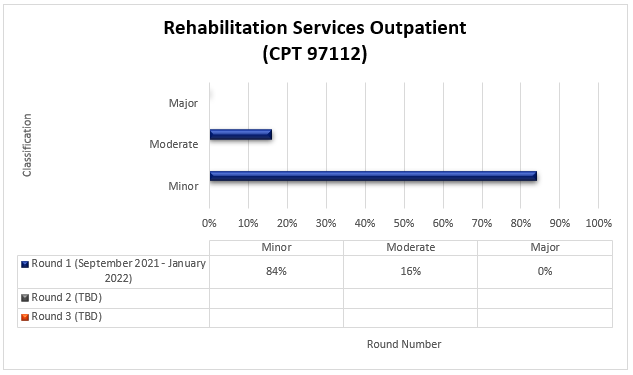
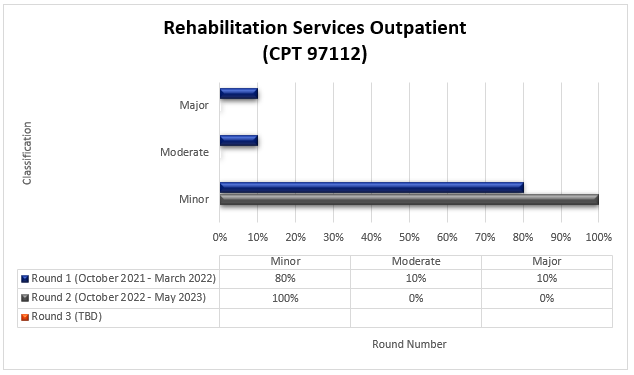
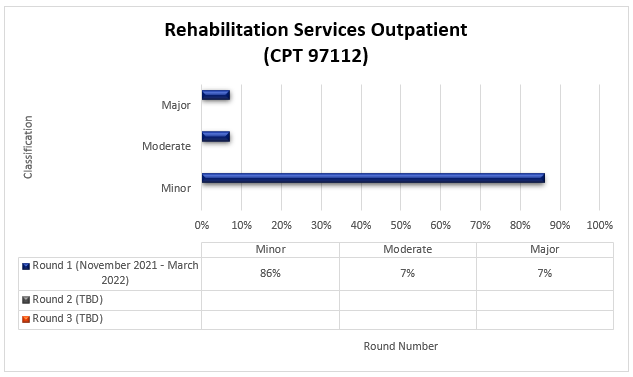
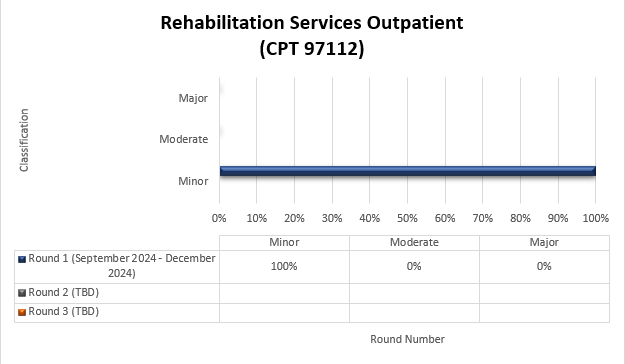
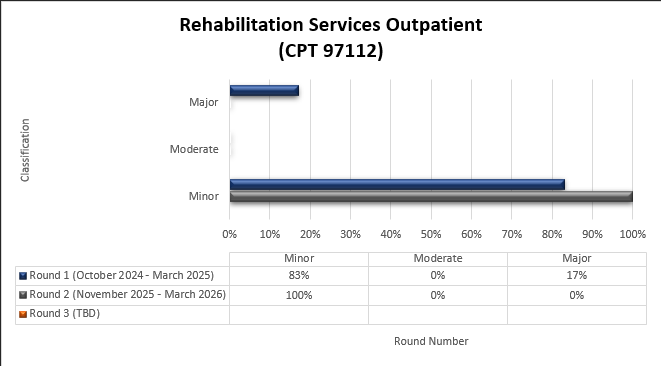
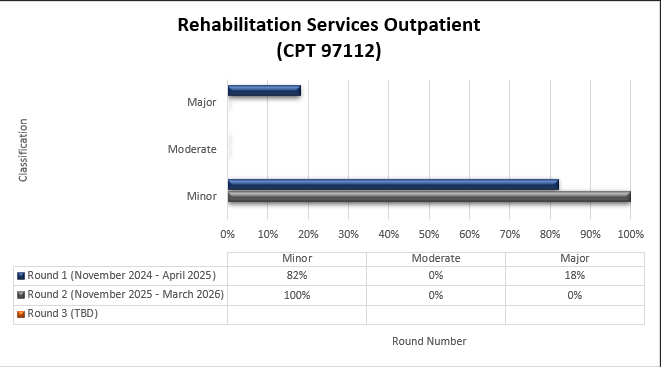
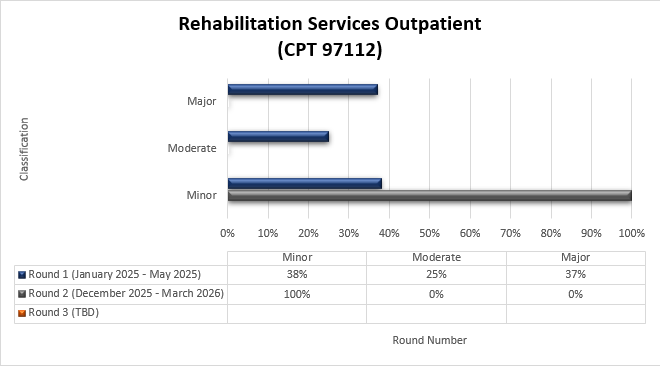
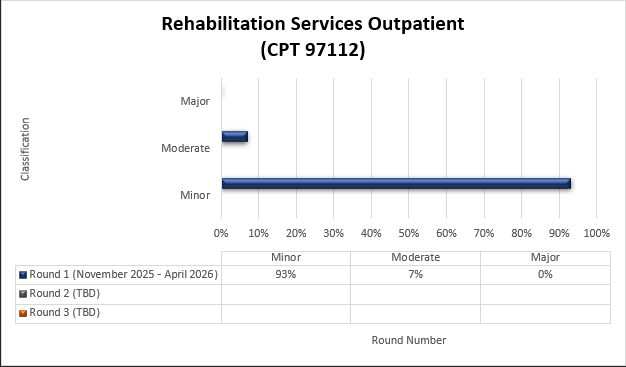
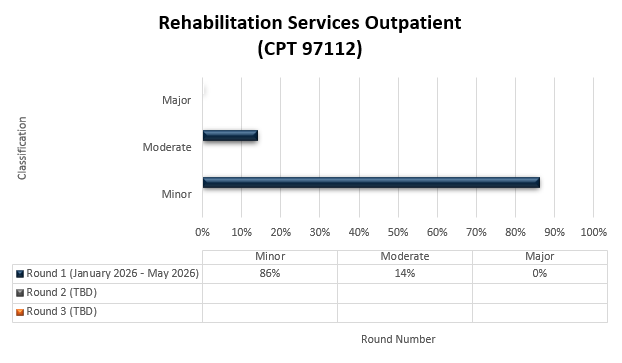
CPT 97112
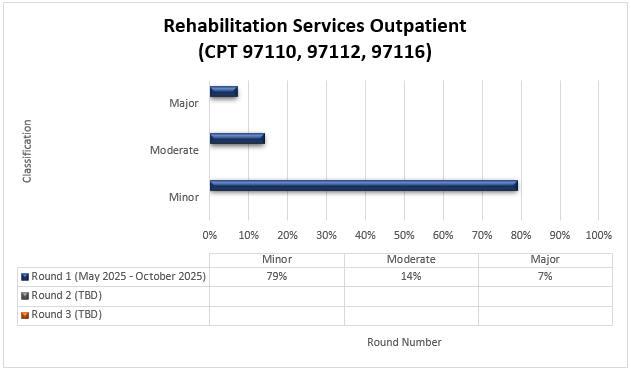
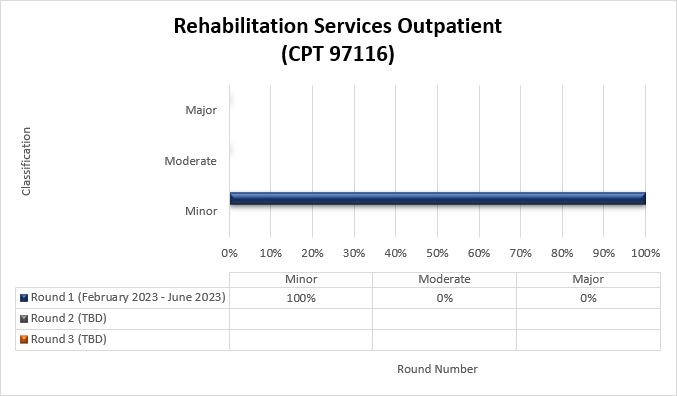
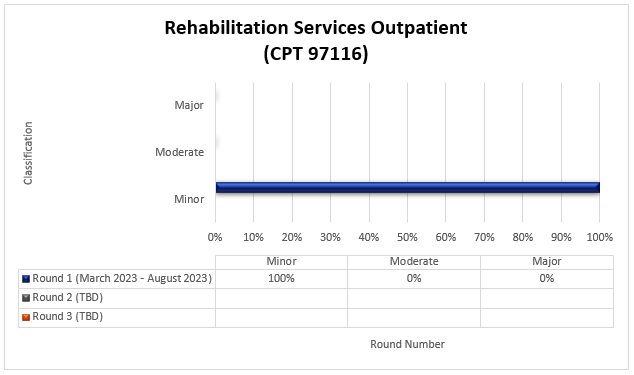
CPT 97116
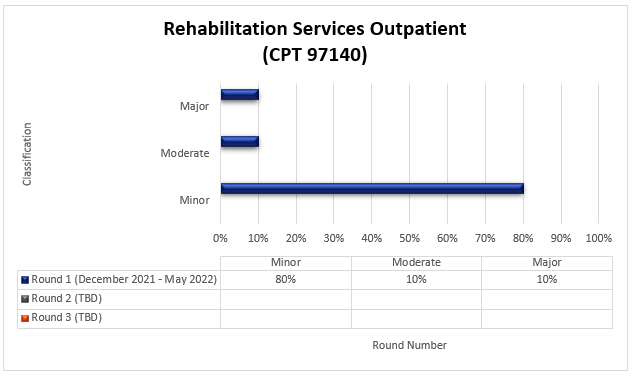
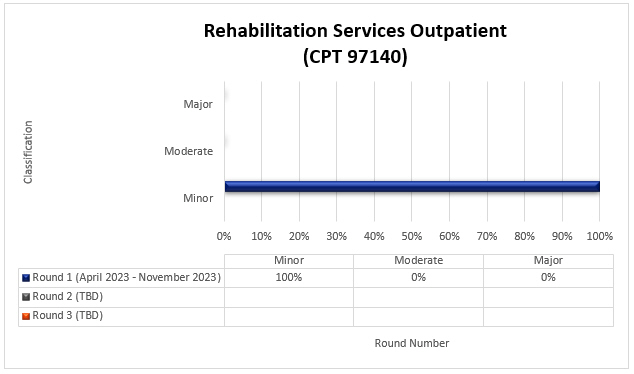
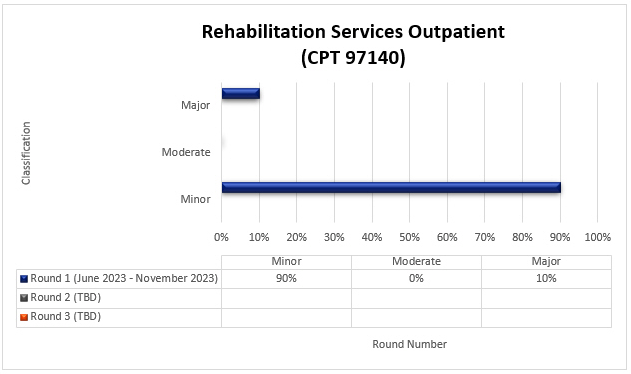
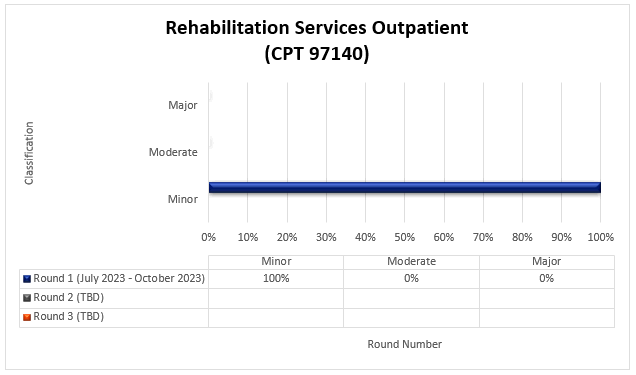
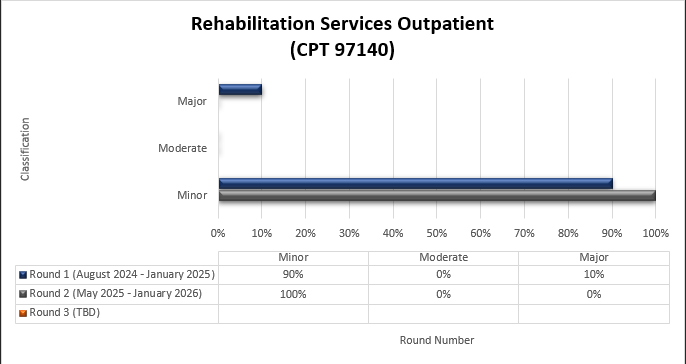
CPT 97140
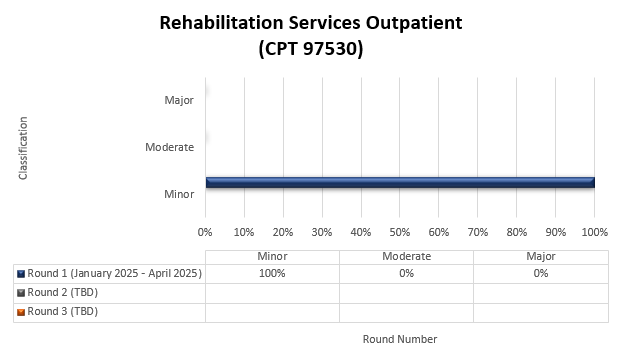
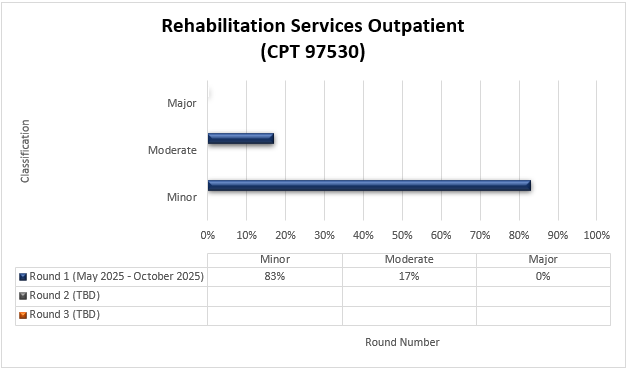
CPT 97530
Multi-code Focus